
Introduction
Therapists are trained to guide others through some of the most complex emotional terrain imaginable. Yet when it comes to running a practice, managing a team, or making high-stakes operational decisions under pressure, most graduate programs offer almost nothing. A peer-reviewed study in The Professional Counselor found that nearly 66% of social work graduate students intended to enter private practice — but none of the schools surveyed taught content on establishing or managing a clinical practice.
That gap is real, and it shows up fast.
Interpersonal instincts developed through clinical work are valuable — but they don't automatically translate into leadership skills. The gap shows up in specific, predictable places:
- Handling staff conflict without defaulting to therapeutic neutrality
- Communicating performance expectations with clarity and consistency
- Delegating effectively rather than absorbing every operational task
- Sustaining personal capacity without burning out the practice leader
What follows is a breakdown of what leadership coaching actually builds in therapists — and why those skills matter more than most practitioners expect.
Key Takeaways
- Clinical training does not prepare therapists to lead practices, manage teams, or make decisions under operational pressure.
- Therapists who own or manage practices are effectively small business operators — and need leadership conditioning, not just clinical competence.
- Leadership coaching builds the skills clinical training skips: communication under pressure, structured decision-making, and self-leadership that moves beyond awareness into consistent action.
- Skipping leadership development produces predictable consequences: staff turnover, reactive management, practice plateaus, and accelerated burnout.
- Leadership coaching delivers compounding returns when treated as an ongoing conditioning process, not a single intervention.
What Is Leadership Coaching for Therapists?
Leadership coaching in this context is a structured professional development process, separate from clinical supervision, continuing education, and therapy. It equips therapists with decision-making frameworks, communication strategies, and performance habits needed to lead themselves and others effectively in a practice environment.
It applies to therapists who:
- Own or manage a private practice (solo or group)
- Hold supervisory roles over clinicians or support staff
- Lead clinical teams in community or organizational settings
- Are navigating professional transitions such as scaling to a group practice model or stepping into an administrative leadership role
The distinction from clinical supervision matters. Supervision addresses case competency, ethical practice, and licensure development. Leadership coaching addresses the professional and operational skills that determine how effectively a therapist leads. The two are not interchangeable.
EVP Leadership's approach makes this distinction explicit: leadership coaching is not therapy for the therapist, and it is not a generic soft-skills workshop. It is a structured conditioning process targeting the behaviors and habits that determine performance in high-pressure, real-world situations.
The firm's 90-Day PressurePoint System works through an Identity Layer (consistency, capacity, character), a Diagnostic Layer (mission clarity, decision integrity, execution discipline, and more), and an Execution Layer — building leadership capacity that holds long after the engagement ends.
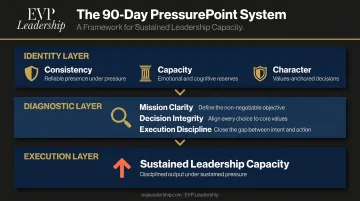
For therapists carrying dual demands — clinical excellence and practice leadership — that kind of structure matters more than inspiration.
Key Advantages of Leadership Coaching for Therapists
The advantages below are grounded in observable, operational outcomes. These are changes that affect how a therapist leads day to day, not just how they think about leadership in theory.
Advantage 1: Structured Communication and Influence Skills
Therapists are highly trained in reflective listening and empathic communication. Those skills are genuinely powerful — inside a clinical context. When a therapist must direct staff, deliver performance feedback, negotiate with referral sources, or communicate a clear vision to a growing team, those same instincts can actually work against them.
Empathic communication optimized for clinical relationships tends to soften direction and prioritize relational comfort over clarity. Leadership coaching builds something different: assertive, goal-oriented communication that complements clinical instincts without replacing them.
In practice, this means deliberate work on:
- Communication framing — structuring messages to reduce ambiguity and prompt action
- Influence without authority — moving people toward outcomes without relying on positional power alone
- Clarity under pressure — sustaining clear, direction-giving language even when conversations are uncomfortable
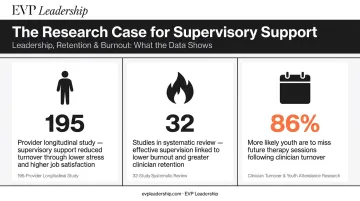
The evidence for why this matters is direct. A longitudinal study of 195 community mental health providers found supervisory support reduced turnover intention through lower work-related stress, lower emotional exhaustion, and higher job satisfaction. A separate mixed-methods systematic review of 32 healthcare studies found effective clinical supervision — anchored in communication quality — was associated with lower burnout and greater staff retention.
Poor supervisor communication doesn't just affect staff. Research shows that clinician turnover directly harms clients: in one study, youth who experienced therapist turnover were 86% more likely to miss a future scheduled therapy session.
KPIs this affects: staff retention, team satisfaction, time-to-resolution on interpersonal issues, client referral rates, practice growth velocity.
When it matters most: during practice growth phases when solo therapists add staff, during performance conversations with supervisees, and when stepping into a clinical director or supervisory role for the first time.
Advantage 2: Decision-Making Frameworks and Practice Leadership Under Pressure
Therapists who own practices are, functionally, small business operators. They manage hiring decisions, cash flow, scheduling systems, credentialing, lease agreements, and growth strategy — often with no formal preparation for any of it.
Most graduate training offers nothing here. APA's 2024 Practitioner Pulse Survey found that among psychologists outside insurance networks, 82% cited administrative burden as a participation barrier — including pre-authorizations, audits, and claims management. Solo and small practices often lack the infrastructure to handle these demands systematically.
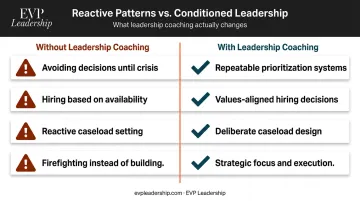
Without structured decision-making habits, practice owners default to reactive patterns:
- Avoiding difficult decisions until they become crises
- Making hiring decisions based on availability rather than fit
- Setting caseloads reactively rather than by design
- Spending disproportionate time firefighting rather than building
Leadership coaching interrupts those patterns by building repeatable systems for prioritization and conditioning deliberate, values-aligned responses before the pressure arrives. EVP Leadership's core thesis — leaders don't rise to expectations, they fall back on their conditioning — holds precisely here. A therapist who has practiced decision-making frameworks in structured coaching is far better equipped to execute under pressure. That preparation shows up during a lease negotiation or a staff departure crisis, not in a calm planning session.
That's what the PressurePoint System is designed to build: Decision Integrity (grounding choices in truth rather than noise and emotion) and Execution Discipline (executing cleanly, consistently, and without unnecessary complexity) — the repeatable operating habits that practice management requires.
KPIs this affects: practice revenue stability, caseload management efficiency, time spent on strategic work versus administrative firefighting, client wait times.
When it matters most: during rapid growth phases, during operational crises, and when a therapist is evaluating a move to a group practice model.
Advantage 3: Emotional Resilience and Self-Leadership Beyond Compassion Fatigue
Therapists understand burnout clinically. The research on compassion fatigue, secondary trauma, and emotional exhaustion is well established in the literature — and most therapists have read it. Understanding the phenomenon, though, is not the same as having conditioned habits that prevent deterioration.
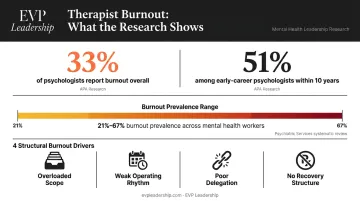
The numbers on burnout in this profession are not abstract. APA's 2024 Practitioner Pulse Survey found roughly one-third of psychologists reported feeling burned out — with the rate climbing to 51% among early-career psychologists within 10 years of completing their doctorate.
A review published in Psychiatric Services found high burnout levels in 21% to 67% of mental health workers across studies, linking burnout directly to staff turnover, absenteeism, and reduced organizational commitment.
Self-care practices help. But they are not sufficient on their own. The structural contributors to burnout — overloaded caseloads, unclear operational limits, poor delegation, no recovery cadence — require leadership-level interventions, not just personal wellness habits.
This is where leadership coaching addresses something therapy does not. It doesn't process the past; it conditions forward-oriented behaviors. Specifically:
- Identifying personal pressure patterns before they produce performance decline
- Building recovery habits into professional routines (not just personal ones)
- Setting operational limits that are clear enough to hold under pressure
- Developing the emotional capacity to sustain consistent performance over time
EVP Leadership's executive burnout recovery work targets the underlying operational drivers — over-scope, weak operating rhythm, poor delegation, no recovery structure — rather than treating symptoms. For therapists, that distinction is the point: a coaching engagement addresses the professional performance dimension that personal wellness habits alone cannot reach.
KPIs this affects: therapist longevity in practice, schedule stability, client satisfaction and retention, supervisory effectiveness.
When it matters most: for therapists carrying high caseloads, managing traumatic content regularly, operating solo practices without peer support, or stepping into larger leadership roles that amplify pressure.
What Happens When Therapists Skip Leadership Development
These patterns show up across practices at every stage — solo, group, and growing:
- Unclear expectations drive turnover — when direction shifts or goes unstated, supervisees fill the gap with their own interpretations. Resentment builds, and exits follow.
- Operational crises consume time that should go toward building sustainable systems. The practice runs the therapist, not the other way around.
- Growth stalls at the therapist's personal capacity — without effective delegation or a communicated vision, the practice has no ceiling except the owner's schedule.
- Accelerated burnout — unclear limits, no conditioned recovery habits, and decision fatigue accumulate. The behavioral health sector already sees approximately 30% annual staff turnover; practices led without operational discipline compound that risk.
- No path to independence — without leadership infrastructure, the practice cannot function when the therapist steps back, takes leave, or tries to expand. Growth becomes structurally impossible.
Each of these outcomes is avoidable — but only if leadership is treated as a discipline to develop, not a byproduct of clinical experience.
How to Get the Most Value from Leadership Coaching as a Therapist
Leadership coaching delivers the highest return when treated as a conditioning process — not a one-time event or a reflective conversation with no follow-through.
Before engaging:
- Clarify the primary focus: communication skills, decision-making discipline, team management, or self-leadership — picking one entry point produces faster traction than trying to address everything at once
- Choose a coach with experience working with practice owners or professionals in service-based fields; generic executive coaching frameworks often miss the clinical context
- Establish clear markers of success before the engagement begins — behavioral changes you can observe and track, not just feelings of clarity
During the engagement:
- Bring specific operational decisions and challenges to each session, not just conceptual questions
- Debrief real situations — a staff conflict, a caseload decision, a difficult conversation — and use coaching to analyze and improve your response
- Practice new approaches between sessions; behavioral conditioning requires repetition outside the coaching hour
Format matters. A structured engagement with a defined timeline and clear phases — Identity, Diagnostic, Execution — keeps progress accountable and measurable. EVP Leadership's 90-Day PressurePoint System is built around exactly that model, designed for practice owners who need operational traction, not open-ended exploration.
The therapists who see the sharpest gains treat sessions as working sessions. Bring real decisions, debrief real situations, and reinforce new behaviors between meetings. That's where the conditioning actually takes hold.
Conclusion
Leadership coaching addresses a concrete skills gap in clinical training — one that shapes how therapists manage themselves, their teams, and their practices under real-world pressure.
Communication clarity, decision-making discipline, and emotional resilience are conditioned behaviors — not fixed traits. They develop through consistent, structured practice and their impact builds over time.
Therapists who are serious about sustainable professional growth should treat leadership development as an ongoing practice, not a one-time seminar. Strong leadership conditioning lifts the quality of every interaction a practice delivers — with staff, supervisees, and clients alike.
Frequently Asked Questions
What are the 7 C's of leadership?
UCLA's Social Change Model defines seven leadership qualities: Consciousness of Self, Congruence, Commitment, Collaboration, Common Purpose, Controversy with Civility, and Citizenship. For therapists balancing clinical and practice leadership, congruence and commitment most directly determine how consistently they lead their teams.
How much does leadership coaching for therapists cost?
Coaching costs vary widely based on the coach's experience, program format, and engagement length. The International Coaching Federation's 2025 Global Coaching Study reported an average of $234 per coaching hour; structured programs like EVP Leadership's 90-Day PressurePoint System use custom engagement pricing. A scoping conversation before committing to any program helps clarify whether the engagement addresses your specific leadership gaps.
Is leadership coaching different from clinical supervision for therapists?
Yes — the two serve distinct purposes. Clinical supervision focuses on case competency, ethical practice, and licensure requirements. Leadership coaching addresses the operational and professional skills needed to lead a practice or team. Both are valuable; neither replaces the other.
Can leadership coaching help therapists prevent burnout?
Leadership coaching targets the structural drivers of burnout: overloaded scope, poor delegation, and unclear limits. It is not therapy, but it directly addresses the self-leadership habits and decision-making patterns that make workloads unsustainable — making it a practical complement to clinical self-care.
What leadership skills do therapists most commonly need to develop?
The most frequent development areas are assertive communication and delegation, structured decision-making under pressure, and building operating systems that allow the practice to function without depending entirely on the therapist's personal availability.
How long does it typically take to see results from leadership coaching?
Meaningful behavioral shifts typically emerge within 60 to 90 days when goals are set upfront and insights are applied between sessions. Open-ended coaching without clear milestones tends to extend that timeline considerably.


